
TL;DR:
- Vitamin K2 activates proteins that direct calcium to bones and prevent arterial deposits, complementing vitamin D’s role in calcium absorption. Combining MK-7 K2 with D3 enhances bone health and reduces cardiovascular risks, especially at higher D3 doses or in low-K2 diets. Taking them with a fat-containing meal ensures optimal absorption, but routine pairing is not mandatory for everyone.
Vitamin K2 is the missing partner in most vitamin D supplement routines because it activates the proteins that tell calcium where to go in your body. Vitamin D increases intestinal calcium absorption from roughly 10–15% up to 30–40%, flooding your bloodstream with calcium. Without K2, that calcium has no clear destination. It can deposit in arteries instead of bones, which is the opposite of what you want. Understanding why K2 with vitamin D matters is not about following a trend. It is about understanding how these two nutrients complete each other’s job.
Why K2 with vitamin D is a calcium traffic problem
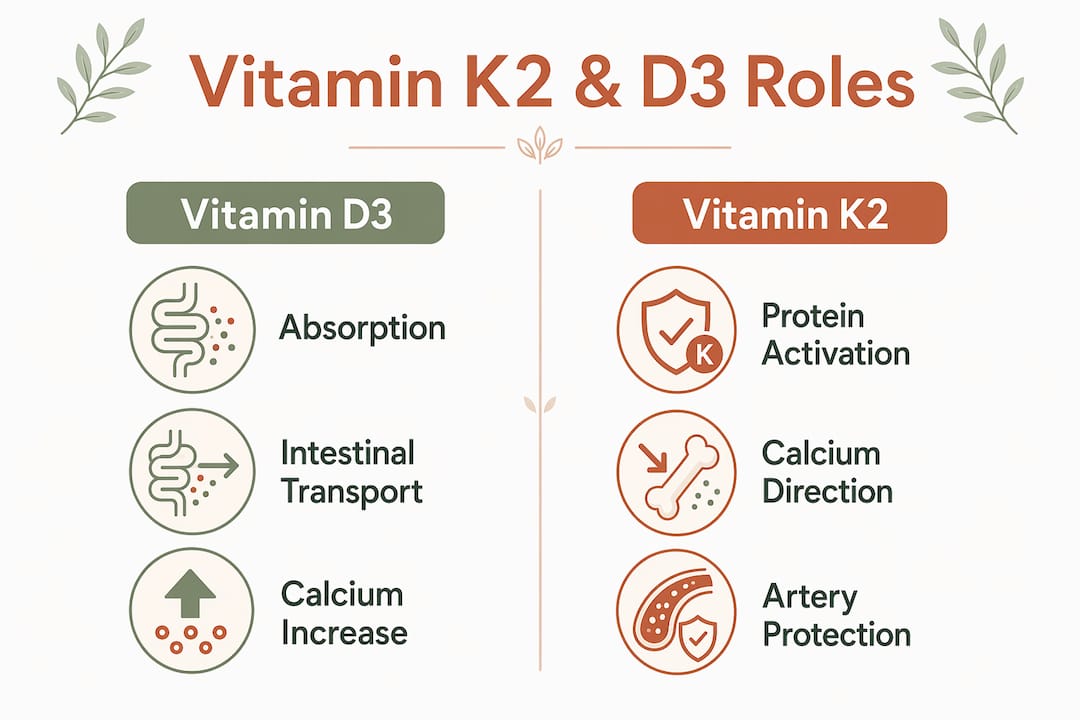
Think of vitamin D as the driver that gets calcium into your bloodstream and K2 as the traffic controller that routes it to the right destination. Vitamin D3, the form your skin synthesizes from sunlight and the form found in most supplements, is the key nutrient for intestinal calcium absorption. When vitamin D levels are adequate, your gut absorbs dramatically more calcium from food and supplements. That calcium then circulates in your blood, waiting to be used.
The problem is that calcium in circulation is not automatically safe or beneficial. Your body needs specific proteins to pull calcium into bone tissue and block it from hardening in soft tissues like arterial walls. Vitamin K2 activates those proteins. Without it, the calcium that vitamin D so efficiently absorbs can end up in the wrong places.
This is not a theoretical concern. High vitamin D intake without adequate K2 has been associated in some studies with increased arterial stiffness, suggesting that the calcium traffic problem is real. The combination of D3 and K2 is sometimes called a “no conflict” pair because they share fat solubility and have complementary biological roles that reinforce each other rather than compete.
What does vitamin D3 actually do for calcium and bone health?
Vitamin D3’s primary job in calcium metabolism is to upregulate transport proteins in the intestinal wall. Without sufficient D3, your body absorbs only about 10–15% of the calcium you eat. With adequate D3, that figure climbs to 30–40% absorbed. That is a two to three times improvement in calcium uptake from the exact same diet.
This matters enormously for bone density. Bones are constantly remodeling, breaking down old tissue and rebuilding with fresh mineral deposits. That process requires a steady supply of calcium. When D3 levels are low, serum calcium drops, and your body compensates by pulling calcium out of bones through parathyroid hormone signaling. The result over years is reduced bone mineral density and increased fracture risk.
Key functions vitamin D3 performs in this system:
- Stimulates calcium-binding proteins in the small intestine
- Maintains serum calcium within the narrow range required for muscle and nerve function
- Signals the kidneys to retain calcium rather than excrete it
- Supports phosphorus absorption, which works alongside calcium in bone mineralization
Pro Tip: If you supplement vitamin D3 but rarely eat calcium-rich foods, you are increasing absorption of a nutrient you are not providing. Pair D3 supplementation with dietary calcium sources like dairy, leafy greens, or fortified foods to get the full benefit.
How does vitamin K2 direct calcium where it needs to go?
Vitamin K2 activates two proteins that are central to calcium placement in the body: osteocalcin and matrix Gla protein (MGP). Osteocalcin and MGP activation by K2 is what separates a calcium-rich bloodstream from a calcium-rich skeleton. Osteocalcin is produced by bone-building cells called osteoblasts. In its inactive form, it cannot bind calcium. K2 carboxylates osteocalcin, switching it on so it can pull calcium into the bone matrix.

MGP works on the other side of the equation. It is expressed in arterial walls and cartilage, and its job is to inhibit calcium from depositing in those soft tissues. MGP also requires K2 to become active. Without K2, MGP stays inactive, and calcium can calcify arterial walls, a process directly linked to cardiovascular disease risk.
| Protein | Activated by K2 | Primary function |
|---|---|---|
| Osteocalcin | Yes | Binds calcium into bone matrix |
| Matrix Gla Protein (MGP) | Yes | Prevents calcium deposits in arteries |
| Prothrombin (clotting) | K1 primarily | Blood clotting in the liver |
The distinction between K1 and K2 is worth understanding. Vitamin K1 primarily supports liver-based clotting functions. K2 specifically targets bone and vascular tissues. Eating leafy greens gives you plenty of K1 but does not reliably raise K2 levels in bone and arterial tissue. This is why K2 supplementation is discussed separately from general vitamin K intake.
The Rotterdam Study, a large prospective cohort following thousands of Dutch adults over 7–10 years, found that high dietary K2 intake was associated with approximately 50% lower risk of arterial calcification and cardiovascular mortality. That is a striking epidemiological signal, even accounting for the limitations of observational data.
Pro Tip: When choosing a K2 supplement, look for the MK-7 form rather than MK-4. MK-7 has a longer half-life, which means once-daily dosing maintains more consistent blood levels compared to MK-4, which clears the body within hours.
Is it mandatory to always take K2 with vitamin D?
No. No universal official recommendation mandates that you must take K2 every time you take vitamin D. This is a nuance that gets lost in supplement marketing. The pairing is physiologically logical and likely beneficial for many people, but it is not a hard requirement for everyone.
The supposed danger of taking vitamin D without K2 is not settled science. Some studies suggest a potential concern at high vitamin D doses, but the evidence is not strong enough to say that standard vitamin D supplementation causes harm in the absence of K2. Context matters significantly here.
Situations where adding K2 to your vitamin D routine makes the most sense:
- You supplement with higher vitamin D doses, such as 2,000 IU or more daily
- You have known cardiovascular risk factors or a family history of arterial calcification
- Your diet is low in fermented foods, grass-fed dairy, or other natural K2 sources
- You have been diagnosed with or are at risk for osteoporosis
- You are postmenopausal, a period when both bone loss and cardiovascular risk accelerate
Conversely, if you eat a diet rich in natto, aged cheeses, and grass-fed animal products, your K2 intake from food may already be sufficient. The supplement conversation is most relevant for people whose diets do not naturally supply meaningful K2. Combined D3 and K2 supplementation may also modulate inflammation and support immune function, adding reasons beyond bone health to consider the pairing.
What are the practical guidelines for taking D3 and K2 together?
Getting the combination right comes down to form, dose, and timing. The framework is straightforward once you understand the fat-soluble nature of both nutrients.
- Choose MK-7 for K2. MK-7 is the preferred supplemental form because its longer half-life supports once-daily dosing. A typical effective range is 100–200 mcg of MK-7 per day alongside vitamin D3.
- Match your D3 dose to your needs. Most adults benefit from 1,000–2,000 IU of D3 daily for maintenance. People with confirmed deficiency may need more under medical supervision.
- Take both with a fat-containing meal. Both vitamins are fat-soluble, meaning absorption improves significantly when taken with dietary fat. A meal containing olive oil, avocado, eggs, or nuts works well.
- Do not stress about timing of day. No evidence supports a specific morning or evening advantage for either nutrient. Consistency matters more than clock time.
- Respect the upper limit for D3. Excessive vitamin D intake above 10,000 IU daily can cause hypercalcemia, a condition K2 cannot prevent. K2 directs calcium but does not neutralize a vitamin D overdose.
| Nutrient | Recommended daily range | Preferred form | Best taken with |
|---|---|---|---|
| Vitamin D3 | 1,000–2,000 IU | Cholecalciferol | Fat-containing meal |
| Vitamin K2 | 100–200 mcg | MK-7 (menaquinone-7) | Same meal as D3 |
For a broader look at combining supplements safely, including how D3 and K2 fit into a full daily stack, it helps to understand which nutrients compete for absorption and which ones work together.
What does the research actually say about combined D3 and K2 benefits?
The mechanistic case for combining D3 and K2 is strong. The conceptual framework is sometimes described as “traffic and destination”: vitamin D drives calcium into circulation, and K2 directs where it lands. This framework is supported by the known biology of osteocalcin and MGP activation.
The epidemiological evidence, anchored by findings like the Rotterdam Study, points in the same direction. High K2 intake correlates with reduced cardiovascular mortality and lower rates of arterial calcification. These are meaningful signals even if they do not prove causation.
Where the evidence gets thinner is in large randomized controlled trials directly testing the combined effect of D3 and K2 versus D3 alone. RCTs confirming combined cardiovascular benefits over D3 alone are limited, which means clinical recommendations currently lean on mechanistic plausibility and observational data rather than definitive trial results.
“The mechanistic rationale for combining vitamin D3 and K2 is well-supported by protein biology and epidemiological data, but large-scale RCTs directly confirming cardiovascular outcomes from the combination remain limited. Practical recommendations currently rest on the strength of the biological mechanism and cohort study findings.”
This gap does not invalidate the combination. It means the science is still catching up to what the biology already suggests. For most people supplementing D3, adding K2 in the MK-7 form is a low-risk, physiologically grounded decision.
Key takeaways
Vitamin D3 and K2 work together because D3 increases calcium absorption and K2 activates the proteins that place that calcium in bones and keep it out of arteries.
| Point | Details |
|---|---|
| D3 drives calcium absorption | Vitamin D3 raises intestinal calcium absorption from 10–15% to 30–40%, flooding circulation with calcium. |
| K2 activates placement proteins | MK-7 form of K2 activates osteocalcin and MGP to direct calcium into bone and block arterial deposits. |
| Pairing is beneficial, not mandatory | No official guideline requires K2 with D3, but the combination is especially valuable at higher D3 doses or with cardiovascular risk. |
| Fat matters for absorption | Both nutrients are fat-soluble; taking them with a fat-containing meal significantly improves bioavailability. |
| Safety limits still apply | K2 does not protect against vitamin D toxicity; staying within 1,000–2,000 IU D3 daily is prudent for most adults. |
Why I think most people are missing the point about K2
People ask whether they need K2 with vitamin D, and the honest answer is: it depends on your dose and your diet. But here is what I find more interesting. Most people who supplement vitamin D are doing so because they are deficient, which means they are likely absorbing more calcium than their baseline diet ever supported. That is exactly the situation where K2 earns its place.
I have seen the conversation get distorted in two directions. One camp says K2 is mandatory and that taking D without it is dangerous. The other dismisses K2 entirely as a supplement industry upsell. Both miss the point. The biology is clear: K2 activates proteins that vitamin D’s calcium surge depends on. Whether your diet already covers that K2 need is the real question.
For most people eating a Western diet low in natto, aged gouda, and grass-fed animal products, the answer is probably no. That is where a well-formulated supplement makes practical sense. When I think about my own supplement routine with #nutribliss, the D3 and K2 combination is one of the few pairings where the mechanism is specific enough to justify the combination rather than just taking each nutrient separately.
If you are supplementing more than 1,000 IU of D3 daily and your diet does not include regular K2 food sources, adding 100–200 mcg of MK-7 is a low-cost, low-risk decision with a clear physiological rationale. Get your vitamin D levels tested annually. Consider your daily vitamin strategy as a whole rather than treating each supplement as an isolated pill.
— GAURAV
Get the D3 and K2 combination right with Nutribliss
Nutribliss formulates its Vitamin K2 + D3 supplement with MK-7 as the K2 source, paired with cholecalciferol (D3) and BioPerine for enhanced absorption. The fat-soluble delivery is designed to work with a normal meal, no special timing required. Every capsule reflects the same science covered in this article: the right forms, the right doses, and the right pairing. If you want to explore the full range of science-backed supplements Nutribliss offers for bone health, cardiovascular wellness, and overall performance, the science behind the formulations is available on the site. This is where the research translates into something you can actually take.
FAQ
What does vitamin D3 and K2 do together?
Vitamin D3 increases calcium absorption from the gut into the bloodstream, while K2 activates osteocalcin and matrix Gla protein to direct that calcium into bones and prevent it from depositing in arteries. Together, they support both bone density and cardiovascular health.
Do you need to take K2 every time you take vitamin D?
No official guideline requires K2 with every vitamin D dose, but the combination is especially beneficial at higher D3 doses or for people with low dietary K2 intake from fermented foods and grass-fed animal products.
What is the best form of K2 to take with D3?
MK-7 is the preferred form of vitamin K2 for supplementation because its longer half-life supports consistent blood levels with once-daily dosing, making it more practical and effective than MK-4.
Can taking vitamin D without K2 be harmful?
Some evidence links high vitamin D intake without adequate K2 to increased arterial stiffness, but this risk is not confirmed at standard supplementation doses. Staying within 1,000–2,000 IU of D3 daily is considered safe for most adults regardless of K2 status.
When is the best time to take D3 and K2?
Take both with a fat-containing meal to maximize absorption, since both are fat-soluble vitamins. No evidence supports a specific time of day advantage, so consistency with meals matters more than clock timing.